
The vegetative nervous system VNS. and the psyche
Emotions and stress can have a negative effect on the heart and circulation and lead to diseases. The vagus nerve, a branch of the vegetative nervous system (see Fig. 4), can trigger psychogenic cardiac arrest. The vagus nerve is responsible for supplying the internal digestive tract, heart and lungs and controls all other internal organs. As already described by Rüegg, the VNS consists of three parts, the sympathetic nervous system, its opponent the parasympathetic nervous system (to which the vagus nerve belongs) and the intestinal nervous system. The latter has over 100 million nerve cells (neurons), much more than are located in the spinal cord. (Rüegg J C, 2003)
6.1 The Vagus Nerve
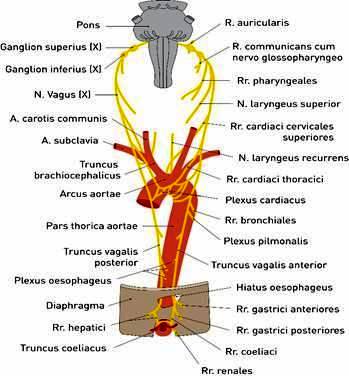
Fig. 4: Vagus nerve
Modified adopted from Plaster R, Pabst R (2000), p. 274
The vagus nerve is the X. It not only has a vegetative function but is also involved in the motor control of various organs such as the larynx, pharynx and upper esophagus. It transmits taste sensations from the base of the tongue and touch sensations from the pharynx, larynx and part of the auditory canal.
6.2 The autonomic nervous system and its two subordinate mechanisms
These include sympathetic nervous system, parasympathetic nervous system and vagus nerve.
Brief anatomical description
The sympathetic nervous system originates from the spinal cord in the chest and lumbar region and continues along the spine. It activates the body for peak performance. As Rüegg already explains, the pulse rises up to five times in the case of an increase in sympathetic activity and blood pressure increases.
In contrast, the parasympathetic nervous system, the opponent of the sympathetic nervous system, can cause cardiac arrest due to its function. Only by harmonizing the sympathetic and parasympathetic nervous systems can regular pulse rates and generally positive organ functions be achieved (Rüegg J C, 2003).
The autonomic nervous system is also known as the autonomous system because its control is involuntary and unconscious. A typical example is mental stress during an oral exam. The sympathetic nervous system works without our will. The stress hormone is increased and blocks the memory areas in the brain. This leads to a temporary interruption of memory (“black-out”) and also to a short-term circulatory disorder of the heart muscle (transient ischemia of the myocardium). This is the case, for example, with an arteriosclerotic narrowing of the coronary vessels, which may lead to a heart attack.
Emotions such as anger, joy, fear, anger, etc. are associated with emotions and manifest themselves in gestures, facial expressions, posture and voice and are also controlled by the VNS. Even the skin blood circulation is emotionally regulated by the sympathetic tone, pallor in the case of a shock or redness in the rage illustrate this process.
Arbitrary or involuntary movements as well as muscle tension or relaxation arise, as already described by Rüegg, through activation of the sympathetic or parasympathetic nervous system and trigger a frequency of electrical impulses (action potentials) (Rüegg J C, 2003).
These are transferred in salvos from the sympathetic nerve cells along the sympathetic nerve fibers to the smooth musculature of the blood vessels or to the heart and heart muscles. In this way, norepinephrine is released by the sympathetic nerve fibers. The frequency rate is 2-8 volleys per second. The overreactions of the sympathetic nervous system cast a kind of mirror image on muscle activity. Moreover, all hand movements, even those that take place only in thought, are activated by the sympathetic nervous system. In an experiment (Vissing and Hjortso, 1996) nerve poison was injected into a forearm to paralyze the muscle. Nevertheless, an activation of the sympathetic nervous system took place during muscle tension. Thus it was proven that this activity was triggered by the brain and not by the muscle tension. For our ancestors, this automated response was an advantage. They were thus well prepared for battle and flight. By comparison, people today live with far fewer combat and escape situations. Unprocessed stress has a negative effect on the cardiovascular system.
The Swiss Nobel Prize winner Walter R. Hess coined the term “defence reaction”. He proved by an animal experiment – weak electric shocks in the hypothalamus, in the lower part of the diencephalon, were transferred to an awake cat – that the cat showed anger and defense behavior and an increase of her blood pressure occurred.
As Rüegg already explains, some involuntary and vegetative body functions, such as body temperature, are controlled by the hypothalamus (cf. Fig. 5). The amygdaloid complex, the corpora amygdaloidea, which is connected to the frontal brain by nerve tracts, monitors the tasks of the hypothalamus. It is also part of the limbic system and lies above the diencephalon (Rüegg J C, 2003).
The corpora amygdaloidea is the place where emotions originate. He evaluates and directs messages coming from the sensory organs, regarding their character, e.g. in dangerous situations, very quickly, even before becoming aware of the danger. Psychosocial stress, which is associated with emotions such as fear, anger and rage, activates the defensive reaction in humans. This is initiated via sympathetic nervous system and hypothalamus.
6.2.1 Division of the brain into its main sections
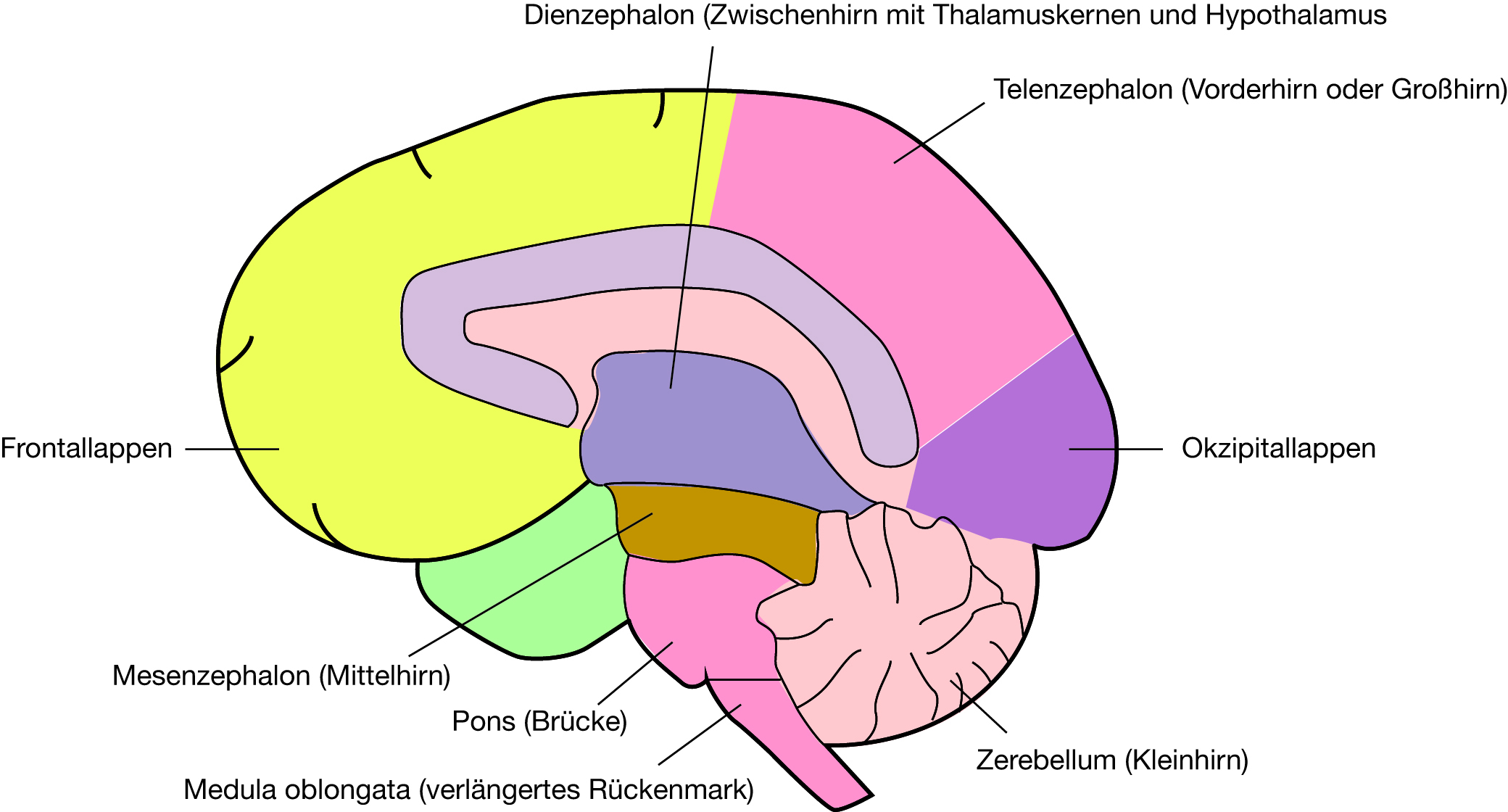
Fig. 5: Division of the brain into its main sections
The left and right cerebral hemispheres of the cerebrum are enveloped by the meninges, in their interior they contain the right and left cerebral ventricles filled with cerebrospinal fluid. Modified taken from: (Rüegg J C, 2003, p.3).
6.2.2 The sympathetic nervous system and its opponent the parasympathetic nervous system
The sympathetic nervous system is activated by unconscious emotional reactions during fighting and defensive reactions, during physical strain, anger and fear.
In humans, the sympathetic nervous system mobilizes the energy reserves in order to achieve exceptional performance. This also activates the cardiovascular system. All organs that are under the influence of the sympathetic nervous system do so simultaneously under the influence of its opponent, the parasympathetic nervous system. This originates in the cruciate marrow, reaches the pelvic organs from there and runs through the spinal marrow to the brain stem. The most important parasympathetic cranial nerve is the vagus, the “wanderer”, which controls not only the heart but the entire digestive tract.
As the term “opponent” suggests, the parasympathetic nervous system, in contrast to the sympathetic nervous system, leads to a recovery phase in the organism. This lowers heart rate and blood pressure.
In harmony between sympathetic and parasympathetic nervous systems, the autonomic nervous system is in a balanced state. In unstable people who suffer from vegetative dystonia, there is an excess of parasympathetic or sympathetic reactions. In the case of a pronounced sympathetic tonus, nervousness prevails. In contrast, as already mentioned by Rüegg, an excess of parasympathetic activity leads to chronic fatigue (Chronic Fatigue Syndrome). The parasympathetic nervous system strengthens the intestinal activity when it is disturbed by the oversized sympathetic tonus. If anger is suppressed, the parasympathetic nervous system can be inhibited. This can lead to constipation
(Rüegg J C, 2003).
6.2.3 Pyramid trajectory system and extrapyramidal trajectory system as part of the vegetative nervous system VNS
Two nerve cords run through the spinal cord: these are the pyramidal tract (descending tract, cf. Fig. 6) and the extrapyramidal tract (ascending tract) of the VNS.
As already Rüegg explains, the nerve cells of the sympathetic branch, which lie in the spinal cord, are excited by neurons in the medulla oblongata (a part of the brain stem) via the pyramid path. The latter in turn is influenced by hierarchically superior brain centres. The pyramidal track is the main part of the pyramidal system (PS). On the lower side of the medulla oblongata the fibres run on both sides of the spinal cord.
Between spinal cord and afterbrain 70-90% of the neurites cross to the other side (pyramid crossing Decussatio pyramidum).
The remaining neurites (Tractus corticospinalis anterior paramedian) run in the anterior strand of the spinal cord and cross into the contralateral side of the spinal cord. The rest remains uncrossed and ipsilateral.
The interneurons in the spinal cord are pulled by the PS and controlled by the motor anterior horn cells. Some fibres form direct connections, the so-called monosynaptic connections (Rüegg J C, 2003).
Pyramid With trajectory system and extrapyramidal trajectory system as part of the vegetative nervous system VNS
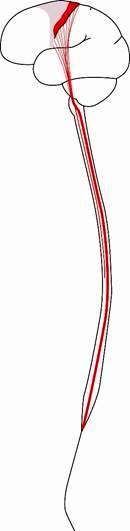
Fig 6: Pyramid orbit system (descending orbit) as part of the vegetative nervous system
Modified taken from: (Kahle W, Leonhardt H, Platzer W, (1979), p. 283).
6.2.5 The autonomic nervous system transmits signals
As described by Rüegg, the spinal cord neurons transmit messages received from the brain via axons (nerval projections) to the so-called sympathetic ganglia, which lie outside the spinal cord.
(see Fig. 7).
The peripheral sympathetic nervous system, the common final distance from the spinal cord to the target organ, consists of chains of two nerve cells each, the preganglionic and postganglionic sympathetic neurons. These are interconnected by synapses (neuronal contacts), which consist of the two cell membranes of the touching neurons and the submicroscopically narrow synaptic gap.
The membrane in front of the cleft is called presynaptic, the other postsynaptic. In the synapse, chemical substances are synaptically transferred from preganglionary to postganglionary nerve cells. The chemical substance, known as acetylcholine, is transmitted and released by electrical impulses (action potentials) when excited via the nerve endings of the preganglionic neurons.
Once acetylcholine molecules have passed through the presynaptic cell membrane, they spread to the opposite side of the synaptic cleft and reach the cell membrane of a postganglionic sympathetic neuron within a thousandth of a second. There, a specific binding to protein molecules of the postsynaptic cell membrane is formed, whereby the acetylcholine receptors adapt to these molecules. If the receptors are occupied by acetylcholine molecules, the receptor molecules are activated and thus the postganglionic neurons are influenced by “depolarisation”. At rest, the cell membranes of these neurons are polarized, i.e. they are positively charged on their outer side and negatively charged electrically on their inner side (ebd.).
The postganglionic sympathetic neurons are electrically discharged by the influence of acetylcholine and trigger action potentials. These are transmitted from the cell body of the neuron in the sympathetic ganglion at a speed of one meter per second to the nerve endings in the sympathetically innervated target organs. Noradrenalin is released, which, as Rüegg explains, is bound to the adrenergic or noradrenergic receptors of the target organs and triggers a noradrenergic organ reaction, for example a vascular constriction, which also occurs when noradrenalin reaches the vascular muscles via the bloodstream.
The sympathetic nervous system and the parasympathetic nervous system consist of two-cell neuronal chains (cf. Fig. 7). In parasympathetic ganglia the interconnection of the pre- and postganglionic parasympathetic cord neurons takes place (ebd.).
6.3 The Peripheral Vegetative Nervous System
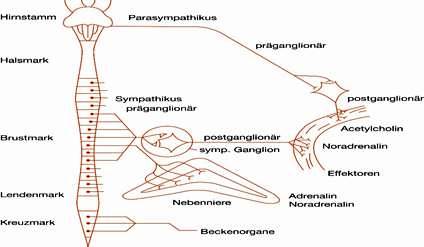
Fig. 7: The peripheral vegetative nervous system
Schematic representation of the peripheral nervous system.
Right: Two-cell neuronal chain in the parasympathetic vagus nerve.
Middle: Schematic representation of the course of a preganglionic neuron of the sympathetic nervous system from the spinal cord to the medulla of the adrenal glands and to the postganglionic neuron which innervates the target organ (e.g. heart or blood vessel). Parasympathetic and sympathetic systems influence the target organs (effectors) by releasing the neurotransmitters (noradrenalin or acetylcholine). The adrenal medulla releases 80% adrenaline and 20% noradrenaline into the blood.
Left: Brain stem and spinal cord with the regions of origin of the sympathetic (lumbar and thoracic) and parasympathetic (cruciate and brainstem) systems. Modified taken from: Rüegg J C, 2003, p. 59
As in the sympathetic ganglia, acetylcholine is responsible for signal transmission. In contrast to the sympathetic nervous system, this neurotransmitter is also released by the postganglionic parasympathetic nerve endings at the successful organs.
As Rüegg already explained, the reaction of acetylcholine at the success organs and in the parasympathetic and sympathetic ganglia occurs with two types of acetylcholine receptors, which are distinguished into nicotinerg and muscarinerg respectively. Nicotine and the fungal toxin muscarin are responsible for these names because they are responsible for the specific excitation of the acetylcholine receptors and can therefore be differentiated pharmacologically. The nicotine acetylcholine receptors are widely scattered throughout the body, both in the parasympathetic and sympathetic ganglia, as well as in the arbitrary muscles and also in the brain. There they mediate the stimulating effect of nicotine.
The muscarinic receptors are mainly located on the membranes of the smooth muscle cells of parasympathetic innervated organs. The parasympathetic transfer of postganglionic neurons to target or effector organs (e.g. the pupil) is completely blocked by atropine. This toxic tropane alkaloid binds to the muscarinic acetylcholine receptors and reduces the effect of the parasympathetic carrier acetylcholine. As the influence of the parasympathetic nervous system decreases, the sympathetic nervous system gains in importance. Strangely, atropine does not inhibit the vasodilatory effect of the parasympathetic nervous system in the male sex organ. It is therefore assumed that other parasympathetic carriers must also be included, presumably the neuropeptide vaso-intestinal peptide (VIP) as well as the gas NO (nitric oxide). Viagra increases the relaxing effect of NO on the smooth muscles of the cavernous body and thus strengthens the erection of the male limb (ibid.).
6.3.1 Adrenal medulla ejects adrenaline
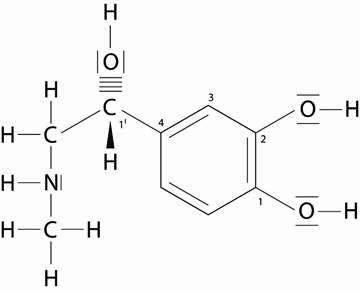
Fig. 8: L-adrenaline: chemical composition of L-adrenaline.
Modified adopted from Löffler G, 2001, p. 481
The formation of adrenaline and noradrenaline takes place in the adrenal medulla. Both are important stress hormones. Adrenaline is also produced in certain nerve cells, the so-called sympathetic ganglia. In the event of a release of adrenaline, noradrenaline is also released in a 4-fold smaller amount. Adrenalin is one of the most important hormones of neurotransmitters and also belongs to the group of catecholamines. Dopamine and norepinephrine also belong to this group and have a similar effect. In case of danger, they transmit signals. Anger and fear activate the sympathetic nervous system and the adrenaline level rises up to 10 times. This activates the metabolic processes and increases the blood sugar level. The blood pressure also fluctuates in time with the pulse and rises to its highest value at each heartbeat (systolic blood pressure). This corresponds approximately to the pressure of a 120 mm high mercury column. Finally, the value decreases and reaches its lowest point (diastolic blood pressure, approx. 80 mm Hg). Pathological blood pressure (hypertension) occurs when the systolic and diastolic blood pressure values exceed 90 to 140 mm Hg in the resting phase (exception: 95 to 160 mm Hg in older people (Andrawis A, 2011).
Medications that have an inhibitory effect on adrenaline and noradrenaline lead to a lowering of blood pressure.
6.3.2 Stress and high blood pressure
In case of danger or threat, a signal and emergency reaction activates the sympathetic nervous system. The adrenal glands react by releasing adrenaline into the blood. As a result, the amount of blood flowing from the heart (the cardiac output) and systolic blood pressure increase. As Rüegg already explained, this happens by increasing the sympathetic tone, because the flow resistance in the circulatory system increases due to a narrowing of the blood vessels. In the case of neurogenic high pressure, an increased frequency of neuronal impulses occurs in the sympathetic nerve fibers. In stressed people, the noradrenaline level is increased and a narrowing of the blood vessels is the result.
The reason is the strong reaction of the vascular muscles to norepinephrine (Rüegg J C, 2003).
Which cell physiolological and molecular mechanisms cause the better signal transmission of noradrenergic synapses between nerve endings and blood vessels in case of overactivation of the sympathetic nervous system?
As already described by Rüegg, the sequence of the impulses (action potentials) in the postganglionic nerve fibers is important for the transmitter release. For this reason, the influence of the sympathetic nervous system increases the flow resistance in the vessel, which increases blood pressure (ebd.).
The number of storage vesicles in the nerve endings is of great importance for signal transmission. How quickly neurotransmitters are replaced and the memory refilled plays an important role. Only 80% of noradrenaline can be released and pumped back into the storage vesicles. The remaining 20% will be replaced by a new synthetic production. Disharmony caused by stress between the activation of the noradrenaline level and the transmitter production via the sympathetic fibres causes a change in the blood plasma (ebd.).
As Rüegg explains, neuropeptide Y (NPY) (acetylcholine and peptidic KO transmitters) is released in the preganglionic nerve endings. Neuropeptide Y causes the increased formation of cyclic adenosine monophosphate (cAMP), an intracellular messenger substance in postganglionic neurons. This leads to an activation of protein kinase, an enzyme that transfers a phosphate group from adenosine triphosphate (ATP) to the tyrosine hydroxylase molecule. ATP causes the phosphorylation process. The result is an optimal regulation of the synthesis of noradrenaline and an adaptation of the content of the available transmitter to the changing conditions of neuronal activity.
This regulatory mechanism takes place not only in the adrenergic neurons of the central nervous system (CNS), but also in the sympathetic ganglia. As a result, the cerebral adrenergic transmission of signals during stress and the tyrosine hydroxyl reactivity in the brain is increased in the long term. The messenger cAMP not only increases the enzymatic activity of tyrosine hydroxyl reactivity, but also the expression of a hereditary factor of the hydroxyülase gene in the cell nucleus, which is responsible for the production of the enzyme, in the case of stress and chronically increased sympathetic tone.
This increases the number of enzyme molecules in the nerve cells and the noradrenaline content in the storage vesicles of the postganglionic neurons increases. This condition is maintained for a few days.
The after-effect of stress lasts for a long time. Thus with each nerve impulse more noradrenalin is released at the sympathetic nerve endings than ever before and the signal transmission from the sympathetic nervous system to the smooth muscles is improved. BP’s rising. In the postganglionic sympathetic neurons, activity-dependent changes have effects on the neuronal plasticity of the CNS or sympathetic nervous system.
The expression (synthesis) of tyrosine hydroxylase also increases in the brain during stress (ibid.).
Univ. Prof. Dr. Andrawis
Bibliography
⦁ Andrawis A (2011): Psychoneuroimmunology (PNI). Complementary Medicine and Holistic Healing. Bachelor’s thesis
⦁ Andrawis A (2013): Psychosomatic Medicine and Psychotherapy, Diploma Thesis
⦁ Andrawis A (2013): The hidden part of the iceberg. A two-year patient analysis, final thesis Specialized in psychoanalysis
⦁ Bridegroom W (2001) theories and practice of psychosomatic medicine in 100 years of its history. In: Deter H C (Ed.) Psychosomatik am Beginn des 21. Centuries. Chances of biopsychosocial medicine. Publisher Hans Huber. Bern. 1st edition
⦁ Bridegroom W, Christian P, by Rad M (1992) Psychosomatic Medicine, a concise textbook. Publisher Thieme. Stuttgart. 6th edition
⦁ Bürgin D, Resch F, Schulte-Markwort M (2009): Operationalized Psychodynamic Diagnostics OPD-2. The Manual for Diagnostics and Therapy Planning, 2nd, revised edition, in German only. Publisher Huber
⦁ Deister A (2005) Reactions to severe stress and adaptation disorders, In: Möller H J, Laux G, Deister A, Psychiatry and Psychotherapy. Thieme Publishers. Stuttgart. 3rd edition
⦁ Deister A (2005) Somatoform Disorders, In: Möller H J, Laux G, Deister A, Psychiatry and Psychotherapy. Thieme Publishers. Stuttgart. 3rd edition
⦁ Dilling H, Mombour W, Schmidt M H (2011): International Classification of Mental Disorders. ICD-10 Chapter V (F). Clinical-diagnostic guidelines, 8th revised edition, Verlag Hans Huber
⦁ Ermann M (2004): Psychosomatic Medicine and Psychotherapy. A manual on psychoanalytical basis, Kohlhammer Verlag
⦁ Fritzsche K, Wirsching M (2006) Psychosomatic Medicine and Psychotherapy. Springer medicine publishing house
⦁ Huber E (2001) Psychosomatic Medicine and the Future of Health Care, In: Deter H C (Ed.) Psychosomatik am Beginn des 21. Jahrhunderts. Opportunities of biopsychosocial medicine, Verlag Hans Huber. Bern. 1st edition
⦁ Kernberg O F (1998): Psychodynamic Therapy for Borderline Patients, Verlag Hans Huber
⦁ Mentzos S (2010): Neurotic Conflict Processing. Introduction to psychoanalytical neuroscience with consideration of new perspectives, Fischer-Verlag
⦁ Möller H-J, Laux G, and Deisster A (2010): MLP Dual Series Psychiatry, Hippokrates Verlag
⦁ Möller H-J, Laux G, Deister A (2014): Psychiatry and Psychotherapy, 5th edition, Thieme Verlag
⦁ Rüegg J C (2003) Psychosomatics, Psychotherapy and Brain. Schattauer Publishers. Stuttgart – New York
⦁ Schuster P, Springer-Kremser M (1997): Building blocks of psychoanalysis. An Introduction to Depth Psychology, 4th edition, WUV-Universitätsverlag
⦁ Schuster P, Springer-Kremser M (1998): Applications of Psychoanalysis. Health and Illness from a Psychoanalytical Perspective, 2nd revised edition, WUV-Universitätsverlag
⦁ Zepf S, (2000): General Psychoanalytic Neuroses, Psychosomatics and Social Psychology, Psychosozial-Verlag
