
Determinants of Decision Behavior from Displacement Healing Faith
„On the importance of early childhood repression in psychoanalysis
And in connection with Christian faith“
In the course of my work as a psychoanalyst and through my many years of experience in the therapeutic field, I have repeatedly observed that patients with a strong belief had a shorter duration of treatment, accepted medication better and could be cured more easily. The established faith attitude seemed to have a significant influence on the better healing process, the deep hope and the confidence in healing in difficult times. In addition to healing, there was also a more rapid reintegration into everyday life, with patients re-establishing relationships and strengthening their social and professional environment. Furthermore, I experienced patients who, due to their lack of religious conviction, had a more difficult course of therapy, which was comparatively longer and more complicated. Based on these observations, it was very important to me to investigate these effects and connections theoretically and empirically. The result of this survey shows that my assumption was correct and that the dissolution of repressed traumas leads to a more peaceful world and good interpersonal coexistence.
The author deals with the following three selected clinical pictures in the research project, which are examined in more detail in Chapter 3 and empirically proven in Chapter 11 – see Andrawis A, (2018).
These would be:
1.) Generalized anxiety disorder F41.1 and DSM-5 Code 300.82
2.) Personality Disorder Borderliner Type F60.31 and DSM-5 Code 301.83
3.) Somatoform disorders-Psychosomatic disorders ICD-10 F. F45. and
DSM-5 code 300.82, (Dilling et. al.2015).
1.2 State of Research
The work deals with the topic of the following criteria: The importance of research into the repressed unconscious and its influence on the improvement of interpersonal relationships and their healing, as well as the early repression of trauma as a cause for the development of mental illnesses. My research project is an interdisciplinary work that combines psychiatric and psychoanalytic methods with Christian beliefs. It is examined whether the Christian attitude has influence on the healing process. The frequency of mental illnesses increases due to traumas that have not been overcome. Efforts for a better understanding of the individual concerned and suitable approaches to therapy are of great importance. Not only for each individual patient, but also for his or her interpersonal relationships.
1.3 Thesis and goal of the work
The results of the research are to be communicated above all to parents and educators, since they are of decisive importance for the education of their children. It is expected that the positive development of the personality and the positive interpersonal relationship will lead to the overcoming of unconscious traumas. For this reason, my study offers a new strategy for the long-term and sustainable relief of those affected and their relatives on the one hand, and forward-looking and preventive health policy on the other. The complete assumption of the costs of psychotherapy by the health insurance funds would be a decisive contribution to public health and public satisfaction.
1.4 Methodological approach
The work is divided into a theoretical and an empirical part. The theoretical part refers to literature research and other international scientific studies. The practical part evaluates the results of a questionnaire interview. The content of the questionnaire asks patients to what extent psychoanalysis and Christian beliefs influence the healing process. The data of the present study were analyzed with a qualitative and quantitative method. The selection is justified and described as well as methodically positioned.
1.5 Outlook
Which preventive measures can be derived from the result of the research question? As the results of the research show, the basic attitude of faith, together with psychoanalysis, has led to a reduction in the intake of medication. The treatment period of the generalized anxiety disorder has also been shortened by the attitude of faith. With the borderline type, therapy and faith have led in a short period of time to the patients becoming able to work, socialize and relate again. With timely therapy, a chronic course of the disease could be prevented. The results have also shown that the majority of test persons would like the health insurance company to cover the therapy costs, and from the point of view of health policy, the entire assumption of costs would be an important contribution to the prevention of serious consequences, such as inability to work.
1.6 Psychoanalysis and Christian Faith in the Healing Process
It has been shown that the Christian attitude of faith has a very high value in the healing process. It thus supports the psychoanalysis procedures for a better healing process. This shortens the duration of the illness and the length of the therapy. The attitude of faith has a very positive effect on the level of trust.
Differences in subjective opinions are presented and more information about the development of the three selected diseases should be provided. Especially after overcoming traumas for the improvement in interpersonal relationships. There is a need for action to strengthen optimism, expectations of a positive course of the disease. Thus, the results should also be used to derive suggestions for prevention, as these could be desired by patients. The Christian attitude to faith may also play a role here. The evaluations of the different clinical pictures lead to a support regarding the need for change of the health system (Filipp & Aymanns 2015).
2 Methodology and empiricism
The data of the present work were analyzed with a qualitative and quantitative method. The selection is justified and described, as well as methodically positioned.
2.1 Qualitative analysis
The questionnaire interview was based on a patient survey. There were open and standardized questions. As presented by Mayring, (2010), the evaluation was carried out according to the standards of quantitative content analysis. Initially, the answers of the subjects were paraphrased and generalized. The classification was carried out on the basis of these results. The allocation and assessment was coordinated and carried out with a second subject with the aim of global categorization.
2.2 Quantitative Analysis
In order to test the hypotheses and the further explorative analyses of the data, frequency analyses were carried out and descriptive statistics (mean values, standard deviations) were listed and graphically substantiated.
The statistical evaluation was carried out using IBM-SPSS© Version 23 for Windows and Excel.
2.3 Positioning of the methodological process
A combination of quantitative and qualitative research design was selected for the method of this study, as hypotheses were established in advance and an explorative approach based on open questions was considered essential and desirable. The quantitative investigation aims at the measurability and quantification of phenomena in order to make a general statement (Flick 2011). The qualitative methodology was chosen because this work should also generate hypotheses and new research approaches (Flick 2011, Przyborski & Wohlrab-Sahr 2010).
.
2.4 Evaluation procedure
The qualitative content analysis is then described as the evaluation process. The special aspect of the qualitative content analysis is explained and the suitability of the method for the result of the surveys of this work is justified. Subsequently, the process model of the qualitative content analysis is described in detail and applied to the evaluations of this work.
2.5 Content analysis for qualitative analysis
The evaluation method of qualitative content analysis positioned by Mayring has established itself as a conventional approach to text analysis (Mayring 2010). This approach characterizes Flick as an adequate method for introspective perspectives gained in an interview (Flick 2011).
The systematic-methodical process is characterized by a custom-made process of analysis. The orientation of the evaluation is based on a process model, which leads to a classification through a beginning paraphrasing, a generalization and a subsequent reduction. In the last step, this is interpreted in the direction of the question (Mayring 2010).
2.6 Hypotheses and questions
The following hypotheses can be made:
I. With regard to the healing process, there were differences in attitude, with regard to the clinical pictures. Due to the rapidly developing and directly recognizable effects of natural and accompanying psychotherapeutic therapies, patients with psychosomatic disorders expect their illness to be cured sooner than in other forms of therapy.
II. There are various ascriptions of causes with regard to the clinical pictures. Somatoform disorders are in a special state of tension with their social environment, which manifests itself in stress. As a result, the entire organism is disharmonized. Due to this a multiple attribution in this area is expected.
III. With regard to the clinical pictures, there are differences in the choice of therapy. It is suspected that patients with somatoform defects choose alternative therapies such as holistic medicine, natural medicine or others. The patients are convinced that their diseases are caused organically. They do not want to admit that their illness is primarily due to a psychological cause.
IV. The clinical pictures of the test persons are different in their presentation and also run under their therapeutic process, whereby the basic attitude is similarly positive.
V. Patients with somatoform disorders, personality disorders and patients of the borderline type as well as patients with generalized anxiety disorder are similar in their choice of therapy because they opt for psychotherapies. They are critical of drug treatments due to the high side effects and fear of possible dependence.
VI. With regard to compliance, a distinction is made in principle between different clinical pictures. If there is acute distress and the success of the therapy with antidepressants is directly noticeable, the effect of the medication is generally shown two to four weeks after the first administration. It was therefore expected that compliance would be high in all clinical pictures.
VII. Differences with regard to the quality and nature of the self-healing powers, the strength, the spirituality and the belief in the self-confidence of the test persons are to be assumed. At the time of the questioning, as well as the explanation of medicines and other therapy forms, the conviction was that the self-healing forces were first identical with nearly all test persons. Only then was there a deviation between the Christian faith and spirituality.
VIII. There are differences between the novelty value of the therapy results and the clinical pictures. Test persons with somatoform disorders have little experience with antidepressants in therapies because they are convinced that their symptoms are only physical and not psychological. Surprisingly, psychotherapy has shown a positive recovery. Patients with a generalized anxiety disorder and borderline type also met with a positive response.
2.7 Sampling/realization of the sample
The surveys were carried out via an online survey and a questionnaire interview. There was no closer therapeutic relationship to the patients. A total of 105 persons agreed to participate in the study. They were divided into three different clinical pictures, including generalized anxiety disorder
F41.1 Personality disorder Borderline type F60.31, somatoform disorders and psychosomatic disorder F45.40, on (Dilling et al. 2011).
2.8 Questionnaire
Based on a literature search by Strobach (2001) and by including additional relevant questions, a separate online questionnaire was developed and optimized and released for the survey of Prof. DDr. Peter Linnert. During the preparation of the questionnaire a reasonable time expenditure of 10-15 minutes was taken into account. Particular importance was attached to the inclusion of open qualitative questions, in particular the question of what role psychoanalysis and Christian faith played in the healing process. The open answers were recorded in writing by the participants. The observations and analyses were carried out and linked at the individual item level. The questionnaire can be found in the appendix of this work:
2.9 The research question
In this work, the author deals with the following research question:
What roles do psychoanalysis and Christian faith play in the healing process?
Building on this, further questions arise regarding the basic framework of the research question:
– What does overcoming early childhood repressions through psychoanalysis mean and what role does the Christian attitude of faith play in the healing process?
– What can be understood by repression-faith-healing?
– Why does the repressed unconscious have a destructive and infantile effect on interpersonal relationships?
– What roles do the amygdala, psychoanalysis and Christian beliefs play in healing and interpersonal relationships?
– Which preventive measures can be derived from the result of the research question?
3 Description of the sample
In total, the online questionnaire was opened 131 times. In 21 cases the persons stopped the survey directly and in five cases after the first two questions. This results in a usable sample of N=105 persons. The specific number of answers per question is indicated by n in each case.
The patients are on average 47 years old (SD=15.42, Mdn=49 years), whereby the youngest person is 21 years old and the oldest person 82 years old (3 persons did not indicate their age). Almost half of the participants live in a partnership as shown in Table 1. Almost one third of the patients (32%) were in a relationship at the time of the survey.
Table 1: Current relationship status (n=101)
| Frequency | Percent | |
| Living in partnership | 48 | 47.5 |
| Separated | 30 | 29.7 |
| Disease-specific | 23 | 22.8 |
Disease-specific details
3. the qualitatively open questions
Following the qualitative content analysis according to Mayring (2010), the open questions from the questionnaire/interview guide were categorised. The resulting categories are presented and discussed simultaneously with the closed questions.
On average, more than two years ago, the people reported to have noticed the complaints for the first time. Concerning the type of complaints, three quarters suffer from mental or psychosomatic illnesses, one person reported suffering from neurodermatitis and sleep disorders. Every second person states that there is at least one person in the family with the same psycho-psychosomatic symptoms (see Table 2).
Table 2 Disease-specific details
| Frequency | Percent | |
| Time of occurrence | 102 | |
| 1 year ago | 19 | 47.5 |
| 2 years ago | 29 | 29.7 |
| Several years ago | 54 | 52.9 |
| Nature of complaints | 104 | |
| Physical | 14 | 13.5 |
| Social environment | 9 | 8.7 |
| Psycho-psychosomatic | 78 | 75.0 |
| Other | 3 | 2.9 |
| Occurrence in the family | 105 | |
| Yes | 52 | 49.5 |
| No | 32 | 30.5 |
| Do not know | 21 | 20.0 |
Most patients sought help in psychotherapy or from a general practitioner, followed by a specialist (see Figure 23).
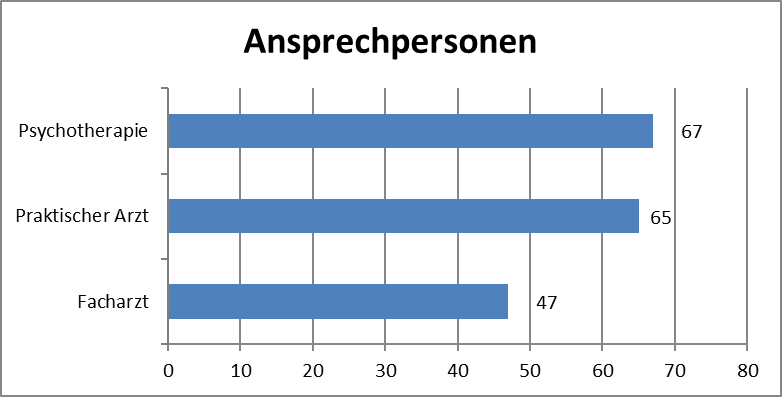
Figure 23: Contact persons (multiple answers, n=179, own representation)
Most patients cited a psychological cause as the reason for their disorder. This is followed by physical causes and the least cited reason, personal behaviour
(see Figure 24).
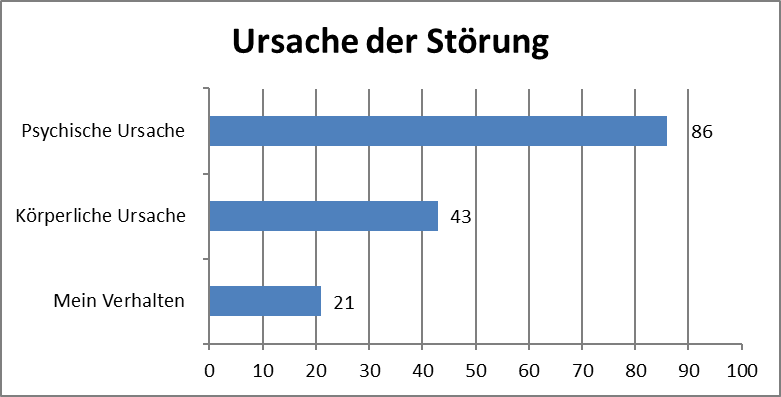
Figure 24: Cause of the fault (multiple answers, n=150, own representation)
69 participants indicated that they would not take any medication for their complaints. In contrast, 35 of those surveyed are currently taking drugs to treat their ailments (see Figure 3).
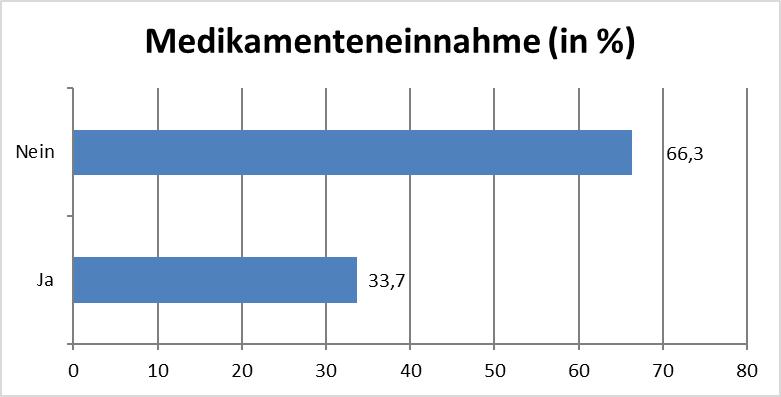
Figure 25: Current medication intake for complaints
(n=104, own representation)
More than three-quarters of the interviewees are optimistic and expect the course of the disease to improve (cf. Figure 26).
Verbesserung des Krankheitsverlaufs (vgl. Abbildung 26).
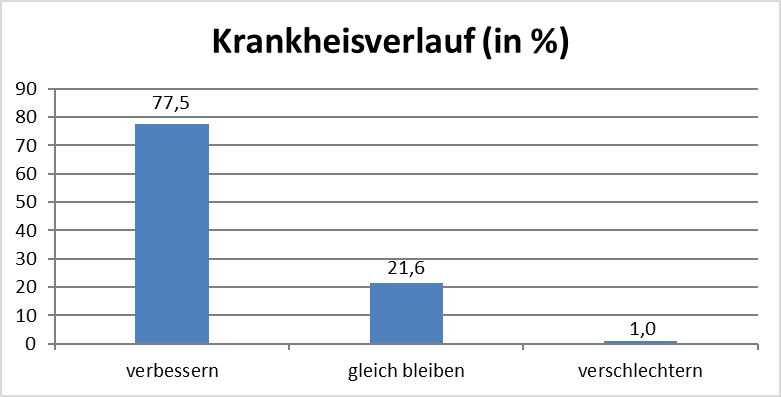
Figure 26 Expected course of disease (n=102, own representation)
On average, people rate the importance of therapies in relation to their own complaints as very important, slightly more than two thirds (cf. Figure 5). The scale was asked from 1 “very important” to 4 “not important at all” and the mean value was M=1.37 (SD=0.61).

Figure 27 Importance of therapies (n=103, own presentation)
88 patients stated that psychotherapy was the most effective way to help them recover. By a large margin, 8 people did not give a measure and 5 participants gave psychotropic drugs as a helpful recovery measure (see Figure 28).
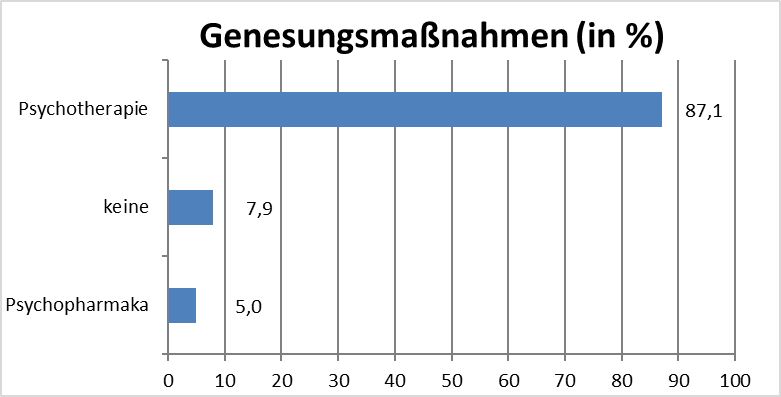
Figure 28: Effective recovery measures (n=101, own presentation)
On average, people rate the efficacy of psychotropic drugs in mental illnesses as effective, which corresponds to 38.8% of respondents. The scale was asked from 1 “very effective” to 4 “not effective at all” and the mean value was M=2.41 (SD=1.06).
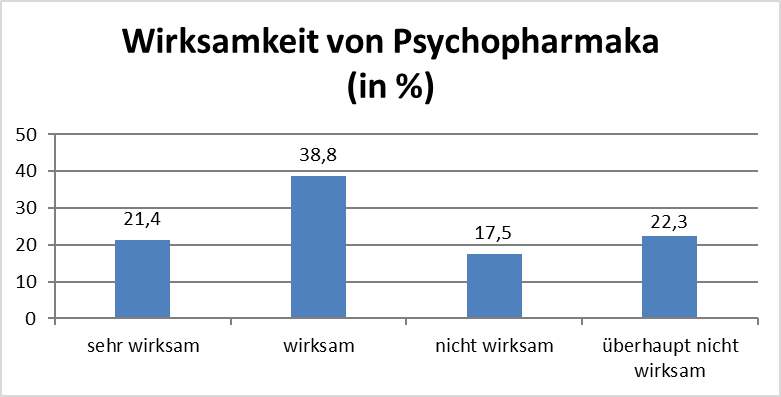
Figure 29: Efficacy of psychotropic drugs in mental illness
(n=103, own representation)
On average, the people rate the handling of their personal illness as good. It is striking that none of the participants stated that they were not at all good at dealing with their own illness (cf. Figure 8). The scale was asked from 1 “very good” to 4 “not good at all” and the mean value was M=2.11 (SD=0.87).
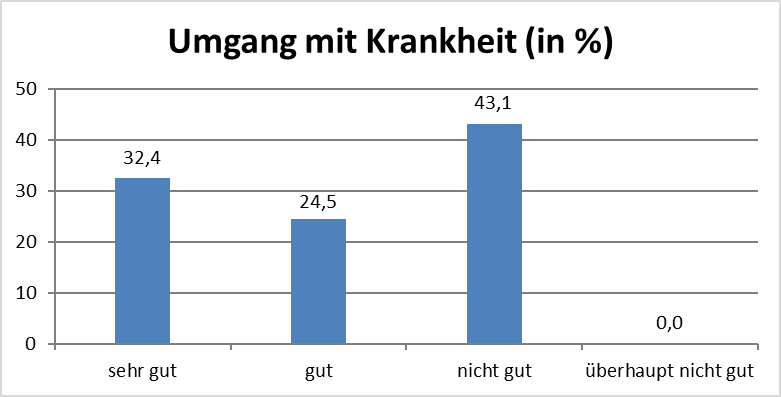
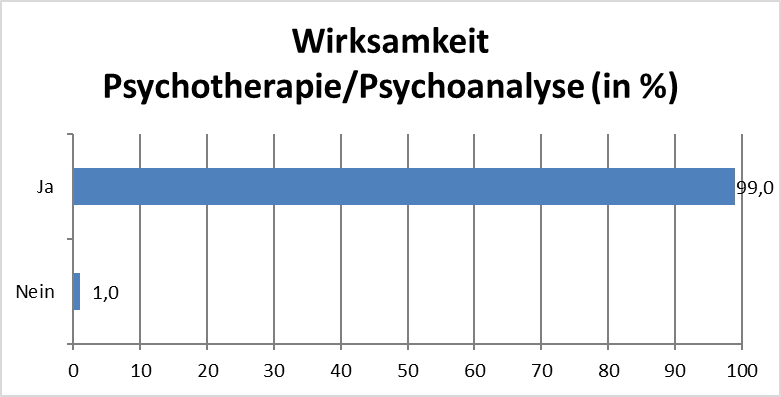
Figure 30: Dealing with one’s own disease (n=102, own representation).
With regard to the open question on the current state of health (see Annex 1, question 16), a total of 105 answers were given. These ranged from a very good condition to a satisfactory or improvable condition to a bad condition with severe current symptoms. With the aim of significantly reducing the information content, a categorization was carried out in line with Mayring’s approach (2010) (cf. Annex 2, Evaluation Table, Question 16). The categorization process took place in two steps, as follows. In the first step, 10 categories were created. From these, 5 categories were aggregated in a second intermediate step (see Table 3).
Table 3: Categorisation of the current state of health
| First step | Number | |
| A | very good | 5 |
| B | good | 20 |
| C | satisfactory | 11 |
| D | has improved | 17 |
| E | healthy | 4 |
| F | stable | 6 |
| G | No complaints | 2 |
| H | in need of improvement | 2 |
| I | bad | 2 |
| J | Acute complaints | 26 |
| Second step | Previous categories | |
| A | very good to good | Category A, B |
| B | has improved | Category D |
| C | Healthy, stable and symptom-free | Category E, F, G |
| D | satisfactory | Category C |
| E | Poor, acute symptoms and in need of improvement | Category H, I, J |
3.1 Perception of psychotherapy/psychoanalysis
Psychotherapy or psychoanalysis is perceived as helpful by 99 patients with mental illnesses. Only one person considers these measures to be unhelpful.
(see Figure 31)
Figure 31: Effectiveness of psychotherapy/psychoanalysis in mental illnesses (n=100, own presentation).
In addition, the patients were asked for their opinion on the assumption of the costs of psychotherapy. More than three-quarters of the patients voted in favour of full reimbursement of the costs of psychotherapy by the health insurance fund (cf. Figure 10).
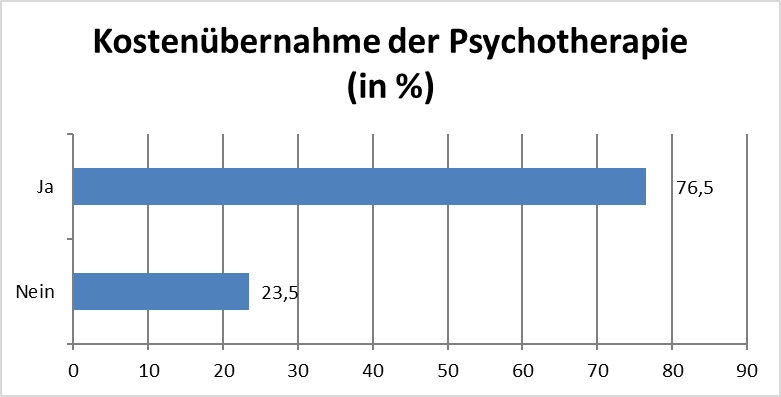
Figure 32: Cost assumption of psychotherapy by the health insurance fund
(n=98, own representation)
3.2 Importance of psychotherapies
The open question on the significance of psychotherapies (see Annex 1, question 18) was answered by 100 patients. These ranged from very helpful and very high value, to low to medium value, to no value at all. With the aim of significantly reducing the information content, a categorisation was carried out following the approach of Mayring (2010) (cf. Appendix 3, Evaluation Table, Question 18). The categorisation process took place in two steps, as follows. In the first, 9 categories were created. From these, 4 categories were aggregated in a second step (see Table 4). The significance of psychotherapies is rated high to very high by the majority.
Table 4: Categorisation of the significance of psychotherapies
| First step | Number | |
| A | Helpful | 1 |
| B | helpful and highly valued | 2 |
| C | medium value | 6 |
| D | unclear, depends on | 3 |
| E | high priority | 23 |
| F | very helpful and very important | 7 |
| G | very high priority | 39 |
| H | helpful and high priority | 5 |
| I | no significance | 2 |
| Second step | previous categories | |
| A | very helpful or very important | Category F, G, J, L |
| B | helpful or highly rated Category | Category A, E, H |
| C | Low to medium value Category | Category C, D, K |
| D | no significance | Category I |
Question-specific analyses
3.3 Patients believe in self-healing powers
Just over 80 of the patients surveyed believe in self-healing powers
(cf. Figure 11)
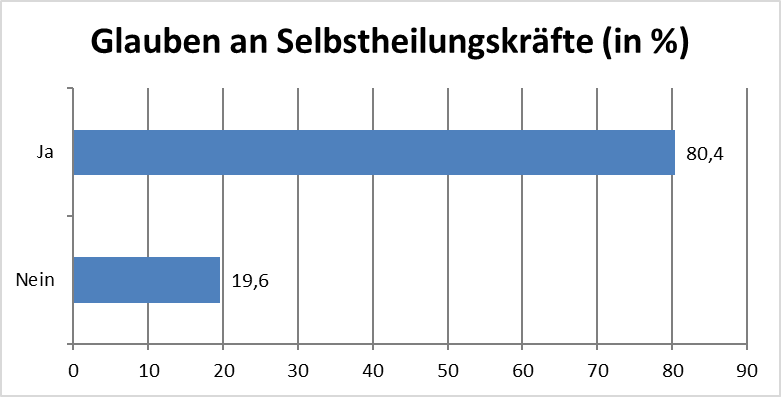
Figure 33 Belief in self-healing powers (n=102, own representation)
The open question about the role of psychoanalysis and Christian faith in the healing process (see appendix 1, question 20) was answered by 95 patients. These ranged from faith plays a (very) big role, psychoanalysis plays a big role and both play a (very) big role until faith leads to psychoanalysis, or a good therapist. With the aim of significantly reducing the information content, a categorisation was carried out following the approach of Mayring (2010) (cf. Annex 4, Evaluation Table, Question 18). The categorisation process took place in three steps, which are as follows. In the first step, 11 categories were created. From these, 7 categories were aggregated in a second step and finally merged into 4 (see Table 5). It can be summarised that both are ascribed a major role.
Table 5: Categorization of the Role of Psychoanalysis and Christian Faith in the Healing Process
| First step | Number | |
| A | Faith plays a very big role | 5 |
| B | Both play a very large role | 16 |
| C | Faith plays a big role | 13 |
| D | Both play a major role | 16 |
| E | Psychoanalysis plays a major role | 9 |
| F | Both play a major role in combination | 8 |
| G | Faith supported, both play a big role | 2 |
| H | Both play a very large role in combination | 10 |
| I | Faith will lead to psychoanalysis (good therapist) | 4 |
| J | Faith supported, psychoanalysis plays a major role | 9 |
| K | no influence | 2 |
| Second step | previous categories | |
| A | Faith plays a (very) large role | Category A, C |
| B | Psychoanalysis plays a major role | Category E |
| C | Both play a (very) large role Category | Category B, D, G |
| D | Both play a (very) big role in combination | Category F, H |
| E | Faith supported, psychoanalysis plays a big role | Category J |
| F | Faith leads to psychoanalysis (good therapist) lead | Category I, L |
| G | no influence | Category K |
| Third step | previous categories | |
| A | Faith plays a (very) large role | Category A |
| B | Psychoanalysis plays a major role | Category B, E |
| C | Both play a (very) big role | Category C, D |
| D | Faith leads to psychoanalysis (good therapist) | Category F |
On average, the persons indicated that they believed that the personal experience of faith had an influence on the healing process. Concerning the existence of a difference between institution and faith, the following were true
85.1% closed. Every sixth person states that he or she does not feel any contribution of faith to recovery. However, 84% of those surveyed said yes to this connection (see Table 6).
Table 6: Faith-relevant details
| Frequency | Percent | |
| Faith Experience Influence on Healing | 99 | |
| Yes | 91 | 91.9 |
| No | 8 | 8.1 |
| Difference Institution and Faith | 101 | |
| Yes | 86 | 85.1 |
| No | 15 | 14.9 |
| Contribution of faith to recovery | 100 | |
| Yes | 84 | 84.0 |
| No | 16 | 16.0 |
3.4 The Open Question on the Contribution of Faith to Recovery
Annex 1 of question 24 was answered by 80 patients. These range from self-determination and self-healing, belief in healing, mental and physical balance to faith, the place of refuge, hope and confidence. With the aim of significantly reducing the information content, a categorisation was carried out following the approach of Mayring (2010) (cf. Annex 5, Evaluation Table, Question 24). The categorisation process took place in two steps, as follows. In the first step, 7 categories were created. From these, 4 categories were aggregated in a second step (see Table 7). Faith is considered to make a considerable contribution to recovery and is regarded by the majority of patients as crucial for the healing process and healing.
Table 7: Categorization of the contribution of faith to recovery
| First step | Number | |
| A | Through self-determination and self-healing | 5 |
| B | By faith in healing | 37 |
| C | Through mental balance (peace, inner voice, security) | 8 |
| D | Through Convinced Faith in Healing | 13 |
| E | By Faith as Refuge, Hope and Confidence | 6 |
| F | By belief in healing and therapies | 10 |
| G | Through mental and physical balance | 1 |
| Second step | previous categories | |
| A | Through self-determination and self-healing | Category A |
| B | By (convinced) faith in healing Category | Category B, D, F |
| C | Through mental and physical balance (peace, inner voice, security) | Category C, G |
| D | By faith as refuge, hope and confidence | Category E |
3.5 Interpersonal relationships after trauma
(see Annex 1, question 25) were answered by a total of 105 persons. The almost exclusively positive answers range from a general improvement via improvements in communication and interaction to enabling an unencumbered new beginning. With the aim of significantly reducing the information content, a categorisation was carried out in line with Mayring’s approach (2010) (cf. Appendix 6, Evaluation Table, Question 25). The categorization process took place in two steps, which are as follows. In the first step, 14 categories were created. From these, 8 categories were aggregated in a second intermediate step (see Table 8).
Table 8: Interpersonal relationships after overcoming trauma
| First step | Number | |
| A | A improved communication | 5 |
| B | harmonic | 7 |
| C | Unloaded | 8 |
| D | Open | 2 |
| E | peaceful coexistence | 22 |
| F | Happy | 4 |
| G | very good | 1 |
| H | New start possible | 5 |
| I | respectful | 0 |
| J | loving | 3 |
| K | Unchanged | 2 |
| L | not answerable | 8 |
| M | better than before | 10 |
| N | understanding | 4 |
| Second step | previous categories | |
| A | A very good or better than before | Category G, M |
| B | peaceful and harmonious coexistence | Category B, E |
| C | unloaded, new start possible | Category C, H |
| D | vImproved and more open communication | Category A, D |
| E | happy, loving | Category F, J |
| F | respectful, understanding | Category I, N |
| G | unchanged, not answerable | Category K, L |
a
3.6 Answering the research question
It has been shown that the Christian attitude of faith is very important for the healing process. It thus supports the psychoanalysis procedures for a better healing process. This also results in a therapy number, a reduction of the duration of the illness and shorter therapy. The attitude of faith has a very positive effect on the level of trust.
3.7 Answering the supplementary questions
Was bedeutet Überwindung frühkindlicher Verdrängungen durch Psychoanalyse und welche Rolle spielt Chr. Glaubenshaltung beim Heilungsprozess?
What does overcoming early childhood repressions through psychoanalysis mean and what role does the attitude of faith play in the healing process?
This means that people have won themselves over to their fellow human beings at the level of interpersonal relationships through self-reflection, empathy, healthy communication and world understanding. The repressed traumas actually have a destructive infantile influence on the pattern of behavior, which manifests itself in the form of reductions, and this is one reason why interpersonal relationships suffer as a result. At this point, the author refers to Chapter I.
3.8 What can be understood by repression-belief-healing
Displacement of all early childhood traumas, including bitterness or injuries, of the current life, which have not been treated but have also been displaced and which manifest themselves as pathological symptoms. This has various influences on the quality of life. Faith lets people trust in itself through their conviction in the dimension of hope for healing and through the natural source of the attitude of faith. This strengthens immunity and leads to a reduction of negative influences. Healing comes through faith and psychoanalysis, both of which have an important role in the healing process.
3.9 The Repressed Unconscious
All repressed human traumas, mostly from early childhood, show themselves in interpersonal relationships through a projection on fellow human beings, which are however unconsciously triggered and carried out. This has an injurious effect on fellow human beings and triggers a very unpleasant feeling. As a result, interpersonal relationships become impossible.
3.10 Amygdala in healing in interpersonal relationships
The amygdala is a center in the limbic system and can be described as the 6th sense. It is the amygdala core and seat of emotion, sometimes also of fear, which makes a significant contribution to interpersonal relationships in which fear plays a major role.
3.11 Which preventive measure can be derived from the result of the research question
As the research results show, basic beliefs and psychoanalysis have led to a reduction in the intake of medication. The treatment period of the generalized anxiety disorder has also been shortened by the attitude of faith. With the borderline type, the therapy and the faith led in a short time to the fact that they became able to work, social and relate again. With timely therapy, a chronic course of the disease could be prevented. The results have also shown that the majority of the test persons would like the health insurance company to cover the therapy costs, and from the point of view of health policy, the entire assumption of costs would be an important contribution to the prevention of serious consequences, such as inability to work, and others, etc…
Univ. Prof. Dr. Andrawis

Klicke hier, um Ihren eigenen Text einzufügen