
Sexuality Function and Psyche
Sexuality functions best in its original, natural and physiological form, with the ability to experience, fantasies, early memories, desires and feelings playing a major role. However, as Fritzsche and Wirsching have already described, there are differences between men and women: the psychological aspect of women influences their entire sexuality. The emphasis is on a good atmosphere and is related to her whole person. Sexuality is different in men. They regard their sexuality as a biological process, coupled with genital-oriented behaviour.
In both men and women, the limbic system and the hypothalamus are responsible for sexuality. The stimulation is triggered by the sensory organs (smelling, seeing, hearing, feeling) and sensitive stimuli. Fantasies and memory are of great importance here (Fritzsche K, Wirsching M, 2006)
Sex hormones
Androgens (androstenedione and testosterone) influence the libido. Both men and women should have a sufficient level of androgen to feel sexual irritability, responsiveness and pleasure. Estrogen is responsible for the increase in libido. Gestagens have a more libido-reducing effect. Estrogens and progestins together, but have less influence than androgens.
Age also has an influence on sexuality. Male sexual excitability and erection strength decreases with age. The male sex organ slackens more quickly after ejaculation and the refraction time becomes longer. In women, the ability to react behaves differently. It generally remains constant, but adapts to the needs of the partner.
When reaching orgasm, men are usually faster than women. In women, however, the climax lasts longer. The subjective well-being of women is more varied than that of men.
Disorders of sexuality
Among the most common disorders in women are vaginismus, lack of interest in sex and orgasm difficulties.
In men, ejaculatio praecox and erection problems are among the main problems.
In most investigations the topic of sexuality remains taboo. As already described by Fritzsche and Wirsching, one should deal with sexual disturbance, lust and dislike. (Fritzsche K, Wirsching M, 2006)
I am of the opinion that the sex drive has an enormous power for the life of a person and plays a big role. Physical complaints are important to consider here: Pelvic area and lower abdomen, especially in older patients, long illness, surgery on the genital organ and problems after a birth.
There are things that accompany us throughout our lives and have a decisive effect on health or illness:
– The healthy emotional bond from childhood onward
– Vulnerability model and stress
– The way to cope with an illness
– Resilience and salutogenesis
Illness and health are relative and consist of an interplay of the patient’s subjective state, his life history, stress resistance, and the strategies for coping with an illness.
Stress
Stress is the condition that can be caused both by physical damage (threatened biological homeostasis or allostasis) and by psychosocial circumstances. The stress reaction is the body’s effort to adapt the biological homeostasis or allostasis by changing the adaptability on the vegetative and endocrine level. Allostasis is the strategy of coping with extreme stresses such as hunger, isolation, extreme temperature fluctuations and prolonged sleep deprivation. Homeostasis establishes the balance between oxygen in the blood, pH and body temperature.
The body does not manage the effort to restore normal behaviour during permanent stress. In the event of temporary stress, this manufacturing process is switched off. The innate protection mechanisms against stress are genetically determined; in some people, as Fritzsche and Wirsching already point out, they can still be damaged by early childhood traumas or loss experiences. (Fritzsche K, Wirsching M, 2006)
Stress during separation in animal behaviour
As Fritzsche and Wirsching have already described, the following reactions occurred immediately after birth after a two-week separation from rat babies: Catecholamine waste, reduction of neocleoproteins, protein synthesis and growth hormones, as well as a reduction of heart and respiratory activity. Moreover, it came to a delayed brain maturation. Sleep disorders occurred and motor activity increased as a result of the predominant parasympathetic inervation. On the other hand, body contact such as stroking and eye contact resulted in a significant reduction of stress. Well-being strengthened the innate defence mechanisms.
The Locus Coeruleus-Norepinephrine (LC-NE axis) and the Hypophysis-Adrenal Cortex axis (HAC axis) play the central role on the organic level in stress reduction. (Fritzsche K, Wirsching M, 2006)
Allostatic overload and stress response
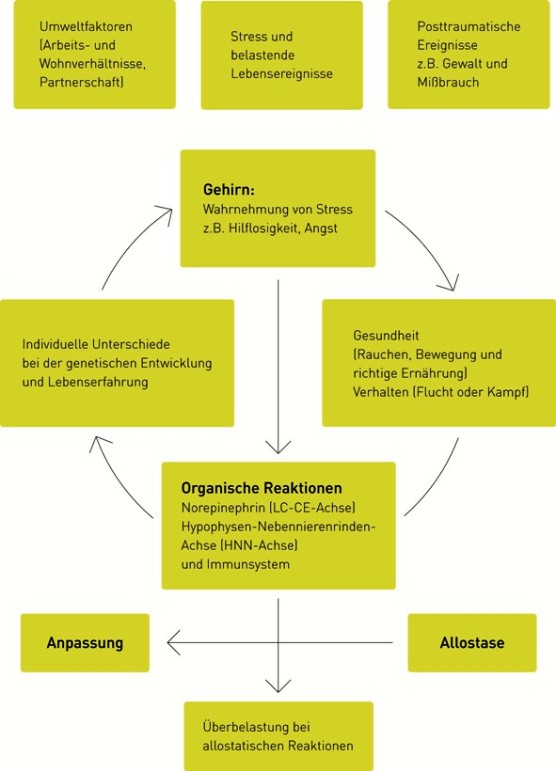
Fig. 3: Overloading with allostatic reaction due to stress.
Modified adopted after McEwen (1998) from Fritzsche K, Wirsching M, 2006, p. 21
Stress also has an influence on bronchial asthma, multiple sclerosis, allergies and rheumatoid arthritis. Stress that lasts between one day and one week leads, as Fritzsche and Wirsching already describe, to an increase in activity on neuropinephrine (LC-CE axis), pituitary adrenal cortex axis (HAC axis) and immune system (IS). The hippocampus plays an important role here. The permanent overload of these mechanisms leads to a dysfunction of the HAC axis and to cognitive stress.
The example shows a stress situation with a partner who suffers from Alzheimer’s and is cared for: Based on studies of influenza vaccination, it was noticeable that fewer antibodies were present in the blood. After years it was proven that the person was more susceptible to disease. Interleukin 6 (IL-6) causes an increase in antibodies in the blood. The hypothalamus-pituitary-adrenal cortex axis has an influence on the cortisol balance. Through the activation of IL-6, the cortisol release is increased and thus leads to the inhibition of the immune system. (Fritzsche K, Wirsching M, 2006)
Stress influences cardiac arrest
A study of 40 patients associated with stress and overuse, especially after severe excitement, such as loss of a loved one, road raid or massive financial loss, showed that catecholamines responsible for stress-related cardiomyopathy were 30 times higher in these people than in healthy people.
In connection with autoimmune diseases, the immune, nervous and endocrine systems are referred to as uniform functions. If one of these systems does not work, the other systems, as already mentioned by Fritzsche and Wirsching, react with a counterregulation. If the stress hormone cortisol cannot fulfil its function, there is an increased risk of inflammation. It’s called an autoimmune disease. Patients with irritations of the HAC axis react with fatigue syndrome and fibromyalgia. (Fritzsche K, Wirsching M, 2006)
Strategies against stress
The interpersonal relationship should be respected at all costs. It plays an important role as a protective factor against overload caused by chronic stress.
– The own mental and physical resilience should not be overstrained.
– Relaxation methods support the vegetative task and influence stress management.
– Stress situations should be avoided as far as possible.
– A healthy diet, sufficient sleep and sport support the body’s own defence mechanisms.
From the point of view of the bond theory, the question can be asked what keeps you healthy and what makes you ill. In my opinion, the experiences of the first six years of life accompany us throughout our lives. The child needs food and warmth, it has the need for emotional attachment, closeness and security. As Fritzsche and Wirsching have already described, if the facial expressions and gestures of the baby are sensitive enough to be maternal/fatherly or emanate from another caregiver, Exytocin is released, which gives the infant pleasant feelings. The amygdala, the hippocampus, the prefrontal cortex and the brain cause a glucorticoid release (CRH) in a stress situation, but this has a protective effect due to the safety of the binding (Fritzsche K, Wirsching M, 2006).
It has been proven that a secure bond increases the resilience to stress and dampens the stress response.
If the mother/reference person does not satisfy the child’s binding needs sufficiently, this results in an uncertain-ambivalent binding behaviour.
An illness of the mother/reference person can lead to a disorder in the development of the child’s stress management system.
The HAC axis is activated by an increased glucorticoid release, which can lead to an elevation of the cortisol level in the blood and thus to damage of the hippocampus. Children suffering from physical or psychological trauma develop hyperreactivity of neuropinephrine (LC-CE axis) and HAC axis.
Psychosocial stress experienced during childhood in particular plays an important role and leads to increased stress vulnerability in later life. It has been proven that alcohol, drugs, fighting or escape behaviour and social withdrawal are effects of these early childhood psychosocial disorders. Smoking, frequent changes of partner and workplace, and deficits in sleep and exercise are also attributed to childhood stress.
Permanent stress leads to physical and mental illnesses.
Psychosocial stress is the triggering factor for 20% of all illnesses.
The next table shows the increased risk of suffering from a mental or physical illness as a result of negative experiences and attachments in childhood. We distinguish between protection and load factors. As Fritzsche and Wirsching already emphasize, protective factors have a balancing effect on the child, strengthen psychological resistance and can absorb negative experiences. In the first three years of life, education and socialisation are directly linked neuronally in the brain. In this way, protective factors can mitigate negative influences on the brain (Fritzsche K, Wirsching M, 2006).
Table 1: This table shows the effects of which positive protective or negative stressfactors contribute to disorders in childhood and adulthood.
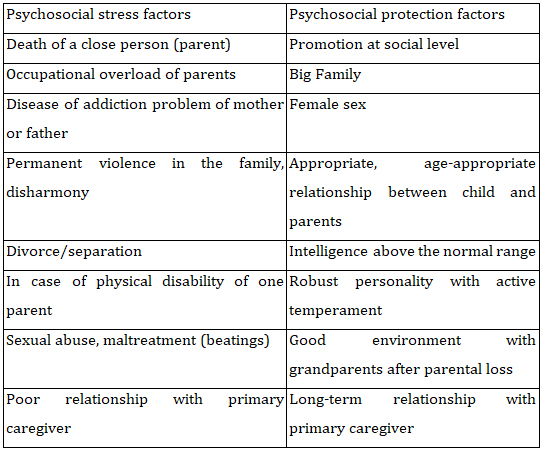
Table 1: Stress and protective factors during childhood
(Fritzsche K, Wirsching M, 2006, p. 24-33)
2.9 Disease processing and Coping
Coping describes the patient’s process of coming to terms with his illness. It includes, as Fritzsche and Wirsching have already explained, all emotional, conscious reactions and the oriented behaviour of the sick person in order to overcome or tolerate problems and strains and to limit feelings of threat in the event of loss of control. The attitude and view of a patient determine the outcome of a disease or life crisis. The patient’s attitude determines which crisis management options are available (Fritzsche K, Wirsching M, 2006).
Three levels of disease management
Behavioral level:
Avoidance, withdrawal, surrender, openness, active cooperation (doctors, nursing staff, …)
Cognitive level:
Acquisition of knowledge about the disease from books, internet, magazines and by psychotherapists. To positively see the threat of the illness through minimalization or through calming sentences: “It will get better, it won’t be anything bad, others have survived it too”.
Affective processing level
from anxiety and grief to psychopathological states: Retreat, panic attacks, aggressive behavior, suicidal behavior, …
Factors influencing the disease:
– Coping patterns learned in life-threatening illness improve stress management. On the other hand, learned helplessness reduces the resistance of the affected person.
– The self-image of the patient influences the view of the disease.
– The way in which physical impairment is dealt with affects the degree of the disease.
– Conscious strategies: seeking social support, gathering general information, social distraction through sport, theatre and cinema,
Search for meaning, religiousness, conversations, walks.
– Unconscious strategies: Defensive mechanisms should help against unpleasant experiences such as diseases and bitterness. Nevertheless, defended thoughts and feelings will emerge as dreams, obsessions, anxiety and depression. (Fritzsche K, Wirsching M, 2006)
The most important defence mechanisms
Denial:
One does not want to admit reality at diagnosis and beginning of a serious illness (e.g. cancer).
Social support:
As Fritzsche and Wirsching already emphasize, it is important that the patient receives social support from persons close to him, the doctor or nursing staff. Patients minimize their disease condition and often present themselves ignorantly. This is where the competent experience of the doctor comes into play, who knows what the patient unconsciously perceived. The doctor does not leave this as it is, but makes the patient aware that there is a denial.
Otherwise, the patient’s trust in the doctor will dwindle, especially and
at the latest, when the disease progresses and the state of the
patients are worsening drastically.
Dissociation:
The patient believes in the inviolability of his body; he considers the presence of disease to be unreal.
Projection:
The patient denies his fear and projects it onto people close to him.
Intellectualize:
Without emotion, purely cognitive and formal, the patient evaluates his situation, sometimes suggests a treatment, e.g. ectomy of the healthy second organ, to maintain the idea of being healed.
Shift and rationalization:
The patient sees the side effects of taking his medication as the trigger of his bad condition. Here is a debt shift (Fritzsche K, Wirsching M, 2006)
The Future of Psychosomatic Medicine in Health Care
Psychosomatic medicine sees the human being as a unit, not only consisting of organs, genes, etc., but also as a whole. Psychosomatics tries to see its actions in terms of the well-being of the human being as a whole in terms of physical, psychological and social aspects. In comparison to genetic engineering, psychosomatic medicine, as Deter already describes, is not only reduced to genes, but sees the human being as a holistic being, embedded in his individual environment or his interpersonal relationships. The human being is part of a communicating system and reacts with adaptation, change, regulation and counterregulation to the requirements of the environment. If it is possible to experience the challenges of the individual as solved, this supports well-being and is beneficial to health. In contrast, a weakening of the entire organism leads to disease. Precisely because psychosomatic medicine does not want to control life, this thought will be of great importance in the future. (Deter H C, 2001)
Univ. Prof. Dr. Andrawis
